
Ulnar Collateral Ligament Treatment Options for Athletes

Many who aren’t throwing athletes may not have heard of the ulnar collateral ligament (UCL), but pitchers, quarterbacks, javelin throwers and others might be intimately familiar with it. It is one of the ligaments of the elbow and is subject to large forces during overhead throwing motions.
Non-athletes may be able to avoid surgery if they injure their UCLs, but overhead throwing athletes may consider surgery to reconstruct or repair a torn UCL to return fully to their sport.
What Is the UCL?
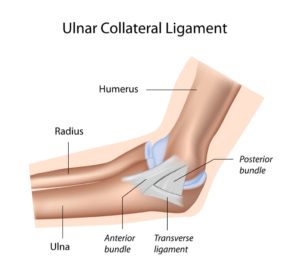 Ligaments connect bones to each other (as opposed to tendons, which connect muscles to bones). The UCL is found on the inside of the elbow (medial side), and it holds the upper arm bone (humerus) to the ulna.
Ligaments connect bones to each other (as opposed to tendons, which connect muscles to bones). The UCL is found on the inside of the elbow (medial side), and it holds the upper arm bone (humerus) to the ulna.
The UCL provides stability to the elbow joint, especially in an overhead throwing motion. Throwing produces valgus forces on the elbow, and the UCL helps to stabilize the elbow from these valgus forces. This means that the ligament is susceptible to injury over time or from a sudden “pop” from valgus force, which can result in a UCL tear.
Symptoms of a UCL Tear
A UCL sprain or tear (a sprain is an injury to a ligament) is usually felt on the inside of the elbow. It can sometimes be mistaken for golfer’s elbow, which is a problem with a tendon that also causes symptoms on the inside of the elbow.
Swelling can also be present in a UCL tear. An audible pop may have occurred if the injury was acute—due to a single event—instead of chronic wear-and-tear. Pitchers, quarterbacks and other throwing athletes may notice a drop in their throwing speed and power, or a loss of control, if they’ve torn their UCL.
Diagnosing a UCL Tear
A physical exam and medical history will be the first steps in diagnosing a UCL tear. During a medical history, athletes’ doctors will be listening for:
- When the pain started
- Changes in training regimen or an increase in volume
- Decreases in throwing speed, power or accuracy
- Any problems with nerves in the area
 A physical exam may involve a number of tests. Doctors will manipulate the arm, looking for signs of pain and ligament laxity (looseness). They may visually inspect the elbow, put it through active and passive range-of-motion tests, check the arm’s strength and stability or feel for any abnormalities in the elbow.
A physical exam may involve a number of tests. Doctors will manipulate the arm, looking for signs of pain and ligament laxity (looseness). They may visually inspect the elbow, put it through active and passive range-of-motion tests, check the arm’s strength and stability or feel for any abnormalities in the elbow.
An X-ray can be useful in ruling out other causes of pain and weakness, such as a fracture, but will not show soft tissue such as ligaments. An ultrasound imaging study can depict laxity in the ligament and show any abnormal thickening. An MRI is the gold standard for evaluating the UCL, and often ordered to evaluate for a UCL tear.
Treatment Options for a UCL Tear
Nonoperative Treatment
Throwing athletes who wish to return to their sport may need surgery for a complete UCL tear. Treatment usually begins—and sometimes ends, especially for non-throwers with no or little laxity—with conservative care.
Nonoperative treatment usually involves rest from throwing for up to six to eight weeks, and then a guided and supervised return to throwing program. Athletes will begin with short tosses, progressing to longer tosses and may end with a simulated game.
A physical therapy program to strengthen both the muscles around the elbow and the entire throwing “kinetic chain,” including the legs and core, will also likely be recommended.

Surgical Treatment
Surgical treatment for a UCL tear has good outcomes in athletes with symptoms of UCL instability. It can include repair or reconstruction. Repair means sewing the ligament back together or re-anchoring it to the bone.
UCL reconstruction is commonly known as Tommy John surgery, after the LA Dodgers pitcher who was the first to have the surgery in 1974. A tissue graft—usually a tendon taken from the patient’s forearm or knee—is threaded through tunnels in the elbow and attached to the UCL. This will act as a scaffold upon which the body will create new connective tissue.
There has been an increase in the number of UCL reconstructions in the last 10 to 15 years. A partnership between youth baseball leagues and Major League Baseball, called “Pitch Smart,” seeks to limit the stress young pitchers put on their elbows and decrease chronic wear-and-tear, hopefully avoiding UCL tears in the future.
Recovery
UCL reconstructions and repairs are usually same-day outpatient surgeries, meaning the patient may leave the hospital or surgical center within 24 hours of surgery with no overnight hospital stay. Procedures in which the surgeon minimizes disruption of the forearm muscles and the ulnar nerve generally have better outcomes.
Initially a splint will be used to hold the elbow in place for up to a week after Tommy John surgery. After that week, the splint will be traded for a brace and range-of-motion exercises can begin. Graduated throwing programs usually start about 10-14 weeks post-surgery, with the goal of returning to play within eight to nine months.
If you are a throwing athlete with a UCL tear or sprain, request an appointment at UOA. Our physicians have an excellent track record of getting our athletes back on the diamond and gridiron after Tommy John surgery. UOA will be with you every step of the way, from initial consultation and diagnosis, to treatment, recovery and beyond.